Oral ulceration
Brief description of the condition
Lesions in the oral cavity or on the lips that are usually, but not always, painful. Ulcers are caused by a number of conditions, most of which are benign (e.g. recurrent aphthous stomatitis, herpes viruses, hand, foot and mouth disease). Other causes include local trauma (e.g. from a sharp cusp, fractured filling, orthodontic appliance or denture), adverse reactions to drugs, nutritional deficiencies, some gastrointestinal diseases and, more seriously, oral cancer.
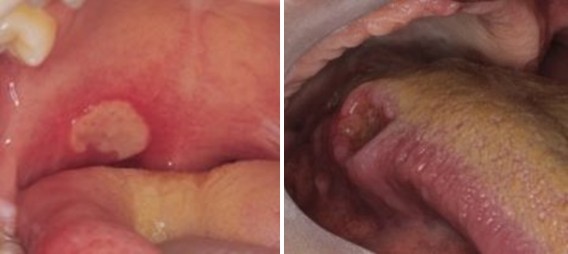
Major recurrent aphthous ulcer (left); Squamous cell carcinoma (right)
Illustrations: LMD Macpherson, J Gibson, VI Binnie, DI Conway, 2003, University of Glasgow Dental School
For other conditions that may present as an abnormal appearance in the mouth, refer to Intra-oral swellings and abnormal appearance.
Key signs and symptoms
- Pain (lips and/or oral cavity)
- Inflammation
- Ulceration
- Abnormal appearance
If the ulceration is severe, some patients (e.g. children, elderly, infirm) may in addition be:
- Listless or agitated
- Dehydrated
Initial management
If a patient presenting with oral ulceration is severely dehydrated, advise the patient or parent/carer to seek emergency medical care.
If there are signs of dehydration (e.g. dizziness/lightheaded, tiredness, dry mouth, lips, eyes) advise the patient or parent/carer to seek urgent medical care.
Do not examine with ungloved hands because of potential infection risk with viral ulcers.
Determine how long the ulceration has been present.
If the ulceration has been present for 3 weeks or more, refer the patient for urgent dental assessment, for possible local Urgent Suspicion of Cancer (USC) referral (oral and maxillofacial surgery) to investigate potential dysplasia or malignancy.36,37
When ulceration has been present for less than 3 weeks:
- If ulceration is recurrent and self-limiting, advise the patient to use 0.2% chlorhexidine* or salt water mouthwash and to seek non-urgent dental care.
- For children, recommend optimal analgesia, soft diet and advise that ulcers are likely to resolve within 1-2 weeks.
- If the patient is receiving drug treatment or has an underlying medical condition that might be the cause of the ulcer(s), advise them to seek urgent medical care (see Underlying medical conditions that may cause oral ulceration and Adverse drug reactions and oral side effects).
- If there are multiple ulcers present, advise the patient to seek non-urgent dental care. However, if the patient is also systemically unwell, advise them to seek urgent medical care.
- If ulceration is due to ill-fitting dentures, advise the patient to use salt water mouthwash, to keep dentures out where possible and to seek non-urgent dental care (also refer to Ill-fitting or loose dentures).
- If there has been trauma from an adjacent tooth or orthodontic appliance, advise the patient to seek non-urgent dental care (also refer to Orthodontic problems).
- If ulceration is likely to be due to trauma to anaesthetised tissue following recent treatment using local anaesthesia, advise the patient to avoid smoking, drinking hot liquids and biting the cheek or lip, and to see a dentist only if symptoms persist or worsen.
- If a single ulcer appears not to have been caused by trauma, advise the patient to use 0.2% chlorhexidine* or salt water mouthwash until symptoms resolve or if the ulcer fails to heal within a week, to see a dentist within 7 days.
- Do not prescribe antibiotics unless there are signs of spreading infection or systemic infection.
In all of the above cases, recommend optimal analgesia, including prescription of topical analgesics such as benzydamine mouthwash or oromucosal spray (see Analgesia).
|
Viral infections |
Primary herpetic gingivostomatitis Hand, foot and mouth disease HIV Chicken pox Herpangina |
|
Bacterial infections |
Syphilis Tuberculosis |
|
Mucocutaneous diseases |
Lichen planus Behcet’s syndrome Pemphigus vulgaris Erythema multiforme Pemphigoid and variants Recurrent aphthous stomatitis |
|
Haematological diseases |
Anaemia Leukaemia Haematinic deficiencies Neutropenia |
|
Gastrointestinal disease |
Coeliac disease Ulcerative colitis Crohn’s disease |
Subsequent care
Consider:
- Fixing ill-fitting dentures if appropriate.
- Prescribing a topical steroid, or a systemic steroid if ulceration is severe.38
- Referring to the local Urgent Suspicion of Cancer (USC) pathway to investigate potential dysplasia or malignancy if ulceration has been present for 3 weeks or more and is unexplained.36,37
- Referral to an oral medicine specialist.
In cases of primary herpetic gingivostomatitis or herpes zoster infection, if the symptoms are severe or the patient is immunocompromised, consider prescribing antiviral agents (see SDCEP Drug Prescribing for Dentistry guidance), ideally in the early stages.
Refer to a general medical practitioner if the patient has an underlying medical condition and is receiving a drug that may be the cause of ulceration.